

.svg)
Modern operating rooms run on extraordinary technology, robotic surgical systems with sub-millimeter precision, AI-assisted imaging that flags anatomy in real time, endoscopic platforms that resolve tissue in 4K.
Yet for many open procedures, surgical illumination is still used the same way it has been for decades: a clunky overhead light that is manually repositioned every few minutes, a fiber-optic cable trailing across the sterile operating room from an external light box, or a head-mounted lamp the surgeon wears for hours.
Today, a different surgical lighting model is taking hold. In-cavity lighting, cordless power, and single-use sterility are converging into a single device. Instead of lighting the entire OR and hoping the light reaches the surgical field, the source goes where the surgeon is already looking: at the retractor tip.
This shift is moving surgical lighting from a somewhat outdated niche specialty solution to a modern, indispensable toolkit reshaping how open surgery is performed.
Effective surgical illumination requires three components: Light must center on the surgeon’s immediate visual field, deliver high-intensity illumination to that field, and penetrate into cavities or under tissue flaps. It seems simple, but none of the existing surgical lighting solutions solve for all three requirements:
Overhead lighting reliably handles the first two for surface-level procedures, but fails on the third.
Headlamps deliver the first and third, but introduce their own tradeoffs (e.g., weight, neck strain, a beam only the wearer sees).
Operating microscopes solve the depth problem only for microsurgery, leaving deep-cavity open work without a default solution.

Figure 1. How the main lighting approaches measure up to modern surgical lighting requirements. Each conventional option falls short on at least one count, while integrated lighted retractors come closest across the board.
These gaps are felt most acutely in tunneled procedures, where surgeons operate through small access points in narrow spaces. In one qualitative survey, 92% of breast surgeons reported not preferring to use headlamps during surgery, citing insufficient illumination in deep cavities, persistent shadows, glare, neck strain, and the risk of contamination. (Cooper et al., 2026, pp. 1-8)
During open procedures, surgical luminaires are repositioned every 7.5 minutes, and the surgeon pauses tasks 97% of the time. (Current State of Surgical Lighting, 2019, pp. 1-8) Unsurprisingly, half of all “sterile” overhead-light handles in one study harbored bacterial cultures, too. (Nosocomial Contamination of Laryngoscope Handles: Challenging Current Guidelines, 2013, pp. 1-4) There’s also the issue of excess heat—fiber-optic cables connecting light sources to retractors or headlamps can reach 437°F in 10 minutes, hot enough to burn through surgical drapes and cause skin burns. (Current State of Surgical Lighting, 2017)
Disposable, battery-powered retractors with integrated LED light sources are the modern design response: by placing the light on the instrument that creates the access channel, illumination enters the cavity at exactly the angle the surgeon needs, and stays where the instrument stays.

Figure 2. Why placement matters. Overhead light is blocked by hands and instruments before it reaches a deep cavity, while an LED at the retractor tip illuminates the field from within.
Instead of routing light from an external source through cables or ceiling mounts to reach the operative field, the design places the LED directly on the instrument that creates the access channel. The light source becomes part of the working tool, not a separate piece of infrastructure that has to be aligned and re-aligned around it.
The market is noticing and responding. The global lighted surgical retractor segment was valued at approximately USD $404 million in 2024 and is projected to grow at a 7.1% CAGR through 2030, driven by demand for minimally invasive and deep-cavity approaches.
The light source becomes part of the working tool, not a separate piece of infrastructure that has to be aligned and re-aligned around it.
Integrating a light source into a retractor creates new design constraints alongside the obvious benefits. The most important technical considerations include:
Precision and brightness: Multi-LED designs let surgeons cycle through configurations—a focused beam for fine dissection, a broader wash for a wider field of view—without repositioning instruments. The conventional external light box, fiber-optic cable, and high-output illuminator remain the benchmark for brightness in procedures that demand maximum lumens at long working distances.
Color temperature and rendering: Correlated color temperature (CCT) refers to the warm-to-cool hue of the beam. Making it adjustable lets surgeons tune the light to the procedure, since no single value suits every operator or operation. The color rendering index (CRI) measures something different: how faithfully the light reproduces true color, which lets a surgeon distinguish oxygenated tissue, fat layers, and pathologic margins.
Sterilization and durability: One review reported that 29.5% of reusable devices tested positive for bacteria even after standard sterilization. (BlázquezGarrido et al., 2018) Single-use integrated retractors eliminate reprocessing entirely, though disposable medical devices generate waste, a sustainability question that remains unresolved for the category.
Heat and risk factors: LEDs at the working end of a retractor avoid the cableheat hazards of tethered systems but introduce a different constraint: the battery and electronics must operate safely with human tissues. Some current ring retractor lighting attachments are engineered to maintain operating temperatures below 38°C.
Device design and user comfort: One-piece design eliminates the need to assemble and disassemble a separate light source, cable, and illuminator. Transferring illumination to the instrument also eliminates a documented occupational health burden: among high-frequency headlamp users, 68% report aggravated neck symptoms (compared with 38% among non- or low-frequency users), and 34% develop clinically diagnosed degenerative cervical disorders (compared to 7%). (Schneider et al., 2024, pp. 830-838)
Integrated lighted retractors have shown the strongest fit in surgical procedures where deep-cavity access, narrow working channels, and shadow-prone anatomy combine to defeat overhead illumination:
Plastic and reconstructive surgery: Lighted retractors are widely used in breast surgery, gynecomastia correction, and other contoured-pocket work, where overhead lights routinely cast shadows into the operative field.
Spine and orthopedic surgery: In-cavity lighting supports minimally invasive and tunneled approaches where the working channel is narrow and deep relative to the access point.
General and abdominal surgery: Hernia repair, cholecystectomy, and other open-pocket procedures benefit from integrated illumination that allows the surgical field to shift in depth and angle.
Colorectal, ENT, and gynecological surgery: Ring-retractor lighting systems have found particular traction here, offering up to 340° of illumination inside deep, narrow wounds.
Ambulatory surgery centers and lower-resource facilities: Sites without access to high-end overhead luminaire arrays can gain access to clinical grade lighting through integrated designs that don’t require additional infrastructure.
The current generation of integrated lighted retractors is the starting point, not the destination. Several developments in modern surgical lighting initiatives and design are converging.
Tissue-Selective Wavelength Control
Targeted LED wavelengths or tunable sources can differentiate vessels, nerves, and pathologic tissue in ways that broadband white light cannot, turning the retractor from a passive light source into an active imaging aid. As wavelength control systems mature, the same instrument holding tissue open could begin to highlight what the surgeon needs to see most.
Multi-Function Integration
Current cordless lighted retractors are absorbing adjacent OR functions:
integrated smoke evacuation channels, suction, and sensor inputs in a single instrument. This reduces the number of separate devices crossing the sterile field, simplifies setup, and consolidates capabilities that previously required multiple connected systems.
Self-Retaining Retractor Pairings
Combining the mechanical advantage of hands-free retraction with integrated or attachable lighting removes two pain points at once: the need for an assistant to hold the retractor and a separate lighting setup. Modular systems that pair selfretaining frames with detachable LED light sources have already reached the market for ENT, colorectal, and gynecological procedures.
AI-Assisted Field Analysis
The modern retractor’s integrated light source can become part of an imaging chain that feeds real-time tissue classification, perfusion assessment, or margin detection back to the surgeon. As real-time AI-driven surgical analysis matures, the device illuminating the cavity may also help interpret what surgeons are seeing.
Currently, unresolved engineering questions in surgical lighting revolve around closing the brightness gap with tethered systems while maintaining acceptable thermal performance, managing waste at scale as single-use volumes grow, and engineering cost structures that make per-procedure economics work for high volume hospitals.
Where Surgeons Look, Light Should Follow
Surgical lighting has spent most of its modern history as a mere means to an end, outdated infrastructure mounted to ceilings, run through cables, worn on heads, kept separate from the instruments doing the actual work.
Modern, integrated lighting is quietly reshaping how open surgery gets done. It removes a recurring workflow interruption, eliminates a documented source of contamination, reduces physical burdens on the surgeon, and delivers clinical-grade illumination to procedures and settings where it has long been hard to achieve. Integrated lighted retractors have transformed the field by integrating lighting into surgical tools, where the surgeon’s attention already is.
Surgical lighting has spent most of its modern history as a mere means to an end, outdated infrastructure mounted to ceilings, run through cables, worn on heads, kept separate from the instruments doing the actual work.


For most of medicine’s history, good clinical light has been hard to come by. A wall outlet, a ceiling mount, and a fiberoptic cable running back to an external box. Wherever the power was, that was where the light stayed. That is where care had to happen.
Battery-powered medical lighting reimagines medical lighting for the modern world. By moving the energy source onto the device itself, rechargeable lithium-ion or lithium-polymer cells powering high-efficiency LEDs, a whole category of lights now delivers clinical-grade illumination with no cord, no box, and no dependence on the room where it is used.
It may sound like a convenience, but portable medical lighting is so much more than that. Untethering light sources also untethers care: surgical-grade illumination can reach a field hospital, a disaster zone, a patient’s bedside, or their skin.
And because the same battery-and-LED platform that lights a surgical cavity can also deliver therapeutic light, portable systems are the rare device category that does double duty, helping clinicians see while helping patients heal.
Untethering light sources also untethers care: surgical-grade illumination can reach a field hospital, a disaster zone, a patient’s bedside, or their skin.
Fixed lighting infrastructure solves one problem well: brightness in a known location. Hang a luminaire array over an operating table, and you get reliable, high-output light exactly where the table sits. The trouble starts the moment care needs to move, or the moment the light needs to reach somewhere a ceiling-mounted beam cannot.
Those limits recur across settings. Cables tether the clinician to a box, creating trip hazards on the sterile floor and adding to setup time. Overhead luminaires light the field from above and behind the surgeon, so the deeper and narrower the surgical pocket, the more the surgeon’s own hands and instruments block the beam.
In more limited settings—including field hospitals, mobile units, rural clinics, and disaster zones—there is often no reliable power, so there is no fixed lighting. Sterility is a quieter liability: reusable corded components are reprocessed between uses, and every reusable part that crosses the sterile field is another potential point of failure to clean and track.
Instead of drawing power from a fixed mains supply, portable lighting devices carry their own power sources. Rechargeable cells drive high-efficiency LEDs for stable brightness, adjustable beam geometry, and extended runtime in a compact, cablefree package. Many designs add status signaling (e.g., battery level, mode changes) so the clinician always knows the device state.

Figure 1. Tethered versus untethered lighting. In tethered lighting models, the light source draws power from a fixed power source. Battery-powered designs place the energy directly on the device, and the light travels with it.
Currently, the category is broad: surgical headlamps, handheld and stand-mounted exam lights, mobile surgical field lights, lighted retractors, and wearable therapeutic light sources. What unifies them is not a shared application but a shared principle, power autonomy:
Power and endurance: Hot-swappable battery modules keep a light running through long procedures without interruption. Charge monitoring is not optional. A portable light without a real-time state-of-charge display risks failing midprocedure, so intelligent control circuits with charge monitoring and external charging capability are essential.
Brightness and optics: High-power LED headlamps reach tens of thousands of lux at typical working distances, with commercial surgical headlights commonly delivering 15,000–30,000 lux, depending on the selected runtime mode. In practice, most portable lights serve as supplemental sources, filling shadows and reaching cavities that overhead arrays cannot, with adjustable spot size and focal length as standard features.
Color temperature and rendering: When surgeons evaluated LED spectra across the 4000–5100 K range, they rated all spectra as effective, with no significant differences, while a warmer 3000 K spectrum was rated lower. The IEC specifies an acceptable range for surgical lighting of 3000–6700 K, with a color-rendering index of at least 85. The same evaluation found statistically significant “spectrum-by-surgeon” preferences, meaning there is no single best color temperature for every operator.
Heat and risk factors: Thermal load is the constraint that scales worst, and more wattage does not automatically buy more useful light. Past a point, added power mainly adds heat, which is why thermal management matters as much as raw output. Engineering responses include heat sinks, liquid cooling, and moving the battery to a waist pack to shift thermal load off the head.
Sterilization and durability: Batteries and electronics cannot survive an autoclave, which forces a design choice. Detachable sterile coverings, sterilizable handles kept separate from the light engine, or fully single-use disposables?
Where fixed lighting is defined by location, portable lighting is defined by its reach. The same untethered platform appears in nearly every setting where care is delivered.

Figure 2. One untethered platform across the care continuum. The same battery-and-LED approach that supplements an operating room also serves the bedside, the field, the home, and on-body therapy.
The operating room: Battery-powered headlamps, handheld field lights, and cordless lighted retractors supplement or replace overhead illumination, bringing light into deep pockets without cables crossing the sterile field. Here, the defining trait is the power source, not the instrument design. The same retractor that another team integrates light into is simply one more device freed from the wall.
The bedside: Handheld and stand-mounted exam lights reveal surface detail, color change, and bleeding patterns that ambient room light washes out, supporting wound assessment and minor procedures for hospital inpatients.
Field, disaster, and military medicine: In austere settings with no fixed power, battery-powered systems are not a convenience but the only option. Military medical support in particular is a pressing need, and recent design work proposes modular, compact lighting that one person can carry to set up a workspace where none existed.
Home and continuous care: Untethered light follows patients out of the clinic, into post-operative monitoring, chronic wound care, and disease management performed in living rooms rather than exam rooms.
Therapeutic delivery: Battery-powered photobiomodulation (PBM) devices— including handheld units, wearable patches, and light-emitting bandages— deliver specific therapeutic wavelengths directly to tissue, a role no fixed luminaire can fill.
The current generation of portable lighting devices is a starting point, but several developments are converging on even smaller, smarter, and more portable light sources. As these devices mature, therapy that once required a clinic visit could run continuously at home.
Flexible, skin-conformable form factors are maturing fast: luminous fabrics that hold stable output over hours of wear with confirmed biocompatibility, OLED-based patches that deliver uniform, low-heat irradiation, and combinatorial dressings that pair nanofibrous wound material with flexible LED arrays. A wearable platform that combines vital-sign sensing with PBM has even been proposed for early treatment of traumatic brain injury in military settings.
The hardest lighting environments—including front-line, disaster, and resourcelimited settings—have historically been an afterthought in luminaire design. That is changing. Recent work directly addresses the lack of specialized lighting for these settings with modular, transferable systems that can be carried, assembled quickly, and run on batteries.
Gesture-recognition controls, the subject of recent patent activity, let a surgeon adjust a sterile headlamp without breaking scrub. (Paul et al., n.d., NIH.gov) Sensorand AI-driven systems aim further ahead, toward optimized surgical lighting that adapts its intensity to the procedure phase, ambient conditions, and the battery state on its own.
Push power autonomy to its smallest scale, and you arrive at fully implantable, wirelessly powered light sources, the domain of optogenetics, where micro-LEDs weighing a fraction of a gram deliver light inside neural tissue. It’s the same engineering problem as a cordless headlamp (miniaturized power, thermal control, biocompatible packaging).
For decades, a patient’s lighting quality depended on the quality of the room they were in. Fixed infrastructure meant fixed geography with fixed limitations. The best medical illumination lived in the best-equipped operating rooms. Everywhere and everyone else had to make do.
By carrying their own power, portable lights bring clinical-grade illumination to the bedside, the field, the disaster zone, and the home. They also increasingly deliver light-based therapies, not just improved visibility.
As batteries shrink, optics sharpen, and controls grow smarter, the question is no longer where good medical light can reach, but rather where we decide to send it.
For decades, a patient’s lighting quality depended on the quality of the room they were in. Fixed infrastructure meant fixed geography with fixed limitations. The best medical illumination lived in the best-equipped operating rooms.


Photobiomodulation (PBM) has everything a breakthrough therapy should, including six decades of research. PBM is non-invasive, well-tolerated, and has a plausible cellular mechanism: specific wavelengths of red and near-infrared light are absorbed by mitochondria, nudging cells toward repair, reduced inflammation, and pain relief.
By every obvious measure, Photobiomodulation (PBM) should be everywhere. But it is not. So the question the field keeps asking is a fair one: Why hasn’t PBM exploded yet?
The answer is that Photobiomodulation is closer than ever to its breakthrough moment. In November 2024, the FDA authorized the first device of its kind, and several bottlenecks that have held PBMs back for half a century are beginning to give way.
In this article, we will take a look at where PBM has earned its place, what has kept it from spreading further, and what is finally starting to change.
Before turning to why PBM has lagged, it helps to be precise about what it does. PBM uses low-level red and near-infrared light, roughly 600–850 nm, at intensities far below those of surgical or ablative lasers. At those wavelengths, light passes into skin and tissue and is absorbed inside by mitochondria, the structures that generate most of a cell’s energy.
The main target is an enzyme in that energy chain called cytochrome c oxidase. When it absorbs the light, the cell’s energy output rises, and a cascade of downstream effects follows: more cellular energy in the form of ATP, reduced inflammation, improved local circulation, and faster tissue repair.
The benefit depends on delivering the right amount of light to the right tissue, a theme that returns as the field’s central challenge.
What PBM does not do is just as important: it does not cut, ablate, or heat tissue. It is a biochemical nudge rather than a thermal one, which is why it is non-invasive and remarkably well tolerated. It is also why dosing is everything. The benefit depends on delivering the right amount of light to the right tissue, a theme that returns as the field’s central challenge.
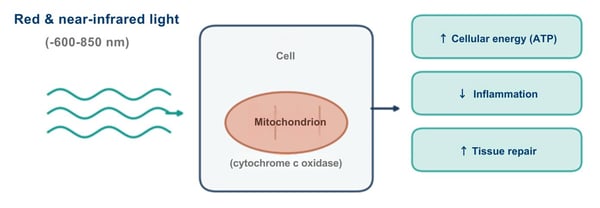
Figure 1. How PBM works. Red and near-infrared light penetrate tissue and are absorbed by mitochondrial cytochrome c oxidase, raising cellular energy and triggering downstream repair and anti-inflammatory effects.
The clearest proof that PBM works lives in oncology. Oral mucositis, the painful breakdown of the mouth's lining, strikes more than half of patients on certain chemotherapy and radiation regimens. (Atwiine et al., 2024, pp. 354-364) It also responds to red and near-infrared light. The evidence is strong enough that PBM receives a full recommendation in the 2020 MASCC/ISOO clinical guidelines for preventing it in patients undergoing head-and-neck radiotherapy and stem-cell transplantation. (Elad et al., 2020, pp. 4423-4431)
This places therapeutic light among the standard supportive-care tools in cancer treatment, and newer work is moving it from the clinic into self-applied, home-use devices. The most consequential recent development, however, came from ophthalmology. In November 2024, LumiThera’s Valeda system became the first FDA-authorized treatment of any kind shown to improve vision in dry age-related macular degeneration, a leading cause of central vision loss for which no prior therapy had been approved.
The pivotal LIGHTSITE III trial randomized 100 subjects, met its primary visual acuity endpoint with multiwavelength light at 590, 660, and 850 nm, and a 2025 extension reported that the gains held with continued treatment. (al., 2026, pp. 1-9) For a field long dismissed as soft, an FDA authorization backed by a shamcontrolled trial is a different order of evidence.
Overall, PBM has a broad, active body of work in wound healing, accelerating repair in diabetic and other slow-healing wounds. (Torkaman et al., 2024, pp. 275-284) It has its largest real-world footprint in pain and musculoskeletal care, the home of most cleared devices and the most familiar face of therapeutic light, though the quality of the evidence varies widely by indication. ((NICE), n.d.)
At the frontier sits transcranial PBM, delivering light through the skull to influence the brain, among the most intriguing directions in the field and among the least settled (it was the subject of a prior edition of this report). (Taylor et al., 2024, pp. 822-827)
The current literature and recent developments on PBM are real footholds. So why does a therapy with guideline backing, an FDA authorization, and 60 years of research behind it not see more use?
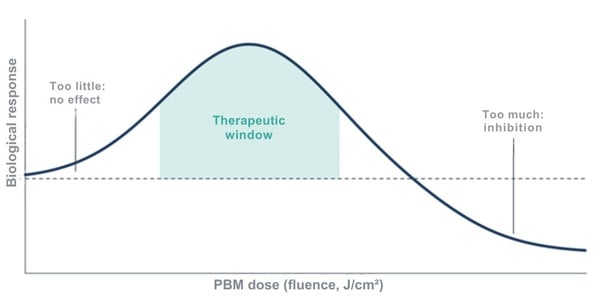
Figure 2. The biphasic or Arndt-Schulz dose response. Too little light produces no effect, while an intermediate therapeutic window yields benefit. Too much suppresses the response, making the correct dose a narrow target.
No consensus dosing: PBM follows a biphasic dose-response, often described by the Arndt-Schulz curve. Too little light does nothing, and too much can actively inhibit the response you wanted. That makes the right dose a narrow target. There is still no consensus framework for defining that therapeutic window across different tissues, depths, and diseases.
Breadth is a liability: PBM appears to help to some degree with an enormous range of conditions, and that scope actually works against it. The field itself identifies the sheer breadth of PBM applications as a credibility barrier. A therapy that seems to treat everything reads, to a skeptical clinician, as one that proves nothing.
Cleared, not approved: Most PBM devices reach the U.S. market through general clearances for broad indications, such as a temporary increase in local blood circulation or relief of minor muscle and joint pain, rather than authorization for a specific disease. The dry AMD authorization stands out precisely because it is the exception.
Reimbursement lags evidence: Even the field’s biggest win is still in progress. Retinal PBM received a Category III CPT code effective January 2025, an emerging-technology tracking code that is a real step toward coverage but not a guarantee of it. Until payers reimburse a use, adoption stays slow regardless of the data.
None of these obstacles is permanent, and none is optical. Standardized dosimetry would make trials reproducible for regulators and payers. The dry AMD authorization gives the next developer a template to follow, one disease at a time. And as clinical grade systems separate from the wellness-gadget market, the credibility drag eases.
The real constraints for PBM were never optical, but rather the absence of standardized dosing, the gap between broad clearance and disease-specific proof, the slow arrival of reimbursement, and the credibility drag of a market full of unproven gadgets.
With the first meaningful authorization on the board and a visible pathway behind it, the next chapter for PBM is about discipline rather than discovery, turning a 60-year promise into routine clinical practice.
The science has been ready for a while. The pieces are starting to line up. And the field is finally catching up.
With the first meaningful authorization on the board and a visible pathway behind it, the next chapter for PBM is about discipline rather than discovery, turning a 60-year promise into routine clinical practice.


Insulin is one of the most important drugs in medicine, and also one of the bluntest. Once injected, it works on its own schedule, not the body’s. Give a little too much, and a patient can slide into hypoglycemia, a drop in blood sugar that ranges from unpleasant to life-threatening.
For a hormone whose entire job is precise regulation—and for the hundreds of millions of people who depend on it—insulin’s lack of fine control is a real limitation.
Now picture a different approach: cells inside the body that produce insulin only when instructed, in measured amounts, on a timescale of minutes, with the onswitch being nothing more than a pulse of light.
That is the premise behind optogenetics. And for diabetes care, the cutting-edge frontier of medical lighting has already moved from idea to measurable results in animal trials.
Now picture a different approach: cells inside the body that produce insulin only when instructed, in measured amounts, on a timescale of minutes, with the onswitch being nothing more than a pulse of light.
Optogenetics is the practice of engineering cells to respond to light, and the basic process is more approachable than the name suggests. A delivery vehicle, often a harmless virus, carries a set of genetic instructions into a target cell. The cell reads those instructions and builds a light-sensitive protein it would not normally produce. When a specific wavelength of light reaches that protein, it flips the biological switch on or off, causing the cell to respond in a specific, pre-engineered way. In this case, the response is increased insulin production.
It’s worth pausing here because this sounds a great deal like Photobiomodulation, the light therapy covered earlier in this report. Photobiomodulation works with the light-sensitive molecules a cell already has, nudging existing biology. Optogenetics installs a brand-new, synthetic switch that the cell never had before. One influences, while the other controls.
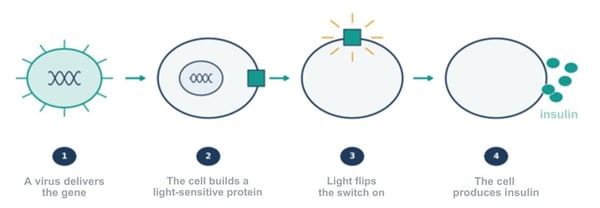
Figure 1. How optogenetics works. A gene-delivery vehicle carries instructions into a cell, which builds a light-sensitive protein. A pulse of light flips the switch, and the cell then produces insulin.
For optogeneticists, precision control is the entire point. Because the switch is engineered, researchers can dictate not just whether a cell acts but exactly when and how much, with a precision in space and time that ordinary drugs cannot match.
Unsurprisingly, optogenetic approaches are under study for eye disease, cancer, and metabolic disorders, but diabetes is where recent momentum is most evident.
A recent generation of light-switchable systems has demonstrated fast, reversible control of insulin in living animals, providing a different order of evidence for a promising mechanism on paper.
REDMAP uses red light around 660 nanometers to activate insulin gene expression. In diabetic mice and rats, light exposure could turn the switch on and lower blood glucose. Red light matters for a practical reason: it penetrates tissue more deeply than shorter wavelengths, so a red switch is an ideal candidate for use beneath the skin.
A second approach uses blue light to drive rapid insulin secretion. While the redlight switch works at a slower level of gene expression, this one acts within minutes. In one study of diabetic mice, insulin levels rose within about 15 minutes of blue-light exposure, and blood glucose returned to a non-diabetic range within an hour. (Chen et al., 2024)
Taken together, the two illustrate an important point. Different wavelengths can be matched to different jobs (e.g., slow and deep vs. fast and shallow), suggesting therapies that could one day be tuned to a patient’s moment-to-moment needs.
For now, these are just animal results. None of this has been tested in humans for the treatment of diabetes. But moving from interesting biology to measurable glucose control on a clinical timescale is exactly the kind of step that propels a viable medical technology toward clinical use.
Several problems remain to be solved before practical optogenetic applications will be ready for human trials, most of them are not about whether the biology works:
Light spectrum: Visible light, especially blue light, does not travel far through tissue. Reaching cells deep in the body with enough light to flip a switch is the field’s central physical obstacle.
Delivery mechanism: Getting the synthetic switch into the right cells, and only the right cells, depends on gene-delivery tools that are still being made safer, both the viral kind and newer non-viral approaches.
Cell engineering: The engineered cells that carry the switch, sometimes called chassis cells, have to remain safe and stable in the body over long periods, which is a high bar for any cell-based therapy.
The optogenetic therapies that have reached clinical trials so far treat neurodegenerative eye diseases such as retinitis pigmentosa, and for a telling reason. In one widely reported case, a patient who had been blind for decades regained partial vision after receiving a light-sensitive protein in the retina paired with a set of light-projecting goggles.
Zooming out, the eye is the ideal proving ground because the retina sits just behind the lens, already built to receive light, which sidesteps the penetration problem entirely. Diabetes, which occurs deeper in the body, is a harder target.
Almost every remaining obstacle to the adoption of optogenetics ultimately comes down to the same question: how do you get the right light to the right cells? The next wave of work is increasingly an engineering problem rather than a biological one.
Currently, two design approaches aim squarely at the depth problem:
Designing light-responsive proteins: These would respond to near-infrared light, which reaches deeper into tissue than visible wavelengths. Upconversion nanoparticles absorb deep-penetrating near-infrared light and re-emit it as visible light that the switch needs, carrying a usable signal where visible light cannot reach.
Stop sending light through tissue at all: Implantable, wirelessly powered light sources can be placed exactly where the engineered cells live, completely solving the penetration problem.
For diabetes, the destination these threads point toward is a closed loop. A wearable sensor measures blood glucose, a controller determines a dose, and a light source signals the engineered cells to release insulin in real time, continuously and noninvasively.
Early versions of exactly this loop have already been demonstrated in diabetic mice, pairing a glucose-sensing component with implanted, light-controlled cells. It would turn diabetes management from a series of manual corrections into something closer to automatic treatment.
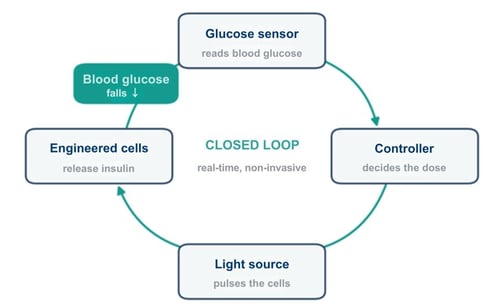
Figure 2. The closed-loop goal for diabetes. A wearable sensor reads glucose levels, a controller sets the dose, a light source signals the engineered cells, and the insulin they release lowers glucose levels.
None of this means insulin injections are going away anytime soon. For diabetes, optogenetics is still early and still pre-human, and the road to the clinic runs through real questions about safety, delivery, and depth. Overpromising would do the field no favors.
But the trajectory here is hard to miss. Medicine has spent a century getting better at identifying and responding to chemical signals in broad, slow strokes. Optogenetics points to something different: control that is precise, reversible, and timed to the second.
Medicine has spent a century getting better at identifying and responding to chemical signals in broad, slow strokes. Optogenetics points to something different: control that is precise, reversible, and timed to the second.

